35 year old female presenting with fever and ulcers on feet and hands since 5 days
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input..
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan .
A 35 year old female, farmer by occupation resident of aakaram came to the general medicine OPD with complaints of fever and ulcers on feet and hands since 5 days
HOPI:
The patient was apparently asymptomatic up until 5 days ago when she developed low grade fever sudden in onset , continuous in not associated with chills,sweating, dizziness, fatigue and body pains, nausea, vomiting .
Second day after onset of fever she went to her farm for work in the early morning and injured her left toe while spraying fertilizer . From third day she noticed progressive painful lesions appearing on both lower limbs and upper limbs chest and neck . Not associated with loss of sensation, itching, joint pains.
Difficulty in swallowing and burning sensation in the mouth post consumption of food due to small ulcers in the mouth
No complaints of headache, burning micturition, giddiness, chest pain, shortness of breath, palpitations, cough ,insomnia, loose stools, loss of appetite.
History of usage of semecarpus anacardium for one day. Following whish she went a local practitioner and was prescribed an tablet containing deflazocort 6mg for five days itraconazole ,tofloxacin, orividazole, clobetalol propionate, and megaheal ointment for five days.
PAST HISTORY and treatment : History of psoriasis vulgaris from 2 years for which she used tab METHOTREXATE 7.5mg BD for one month and capsule itraconazole.
Not a known case of DM/HTN/ TUBERCULOSIS/ASTHMA/
PERSONAL HISTORY:
Appetite: decreased
Diet:mixed
Sleep: adequate
Bowel and bladder are regular
Patient denies of any addictions
FAMILY HISTORY:
no history of similar complaints within the family
General examination
Pallor: present

Icterus:absent
Clubbing: absent
Cyanosis: absent
Lymphadenopathy: absent
Edema: absent
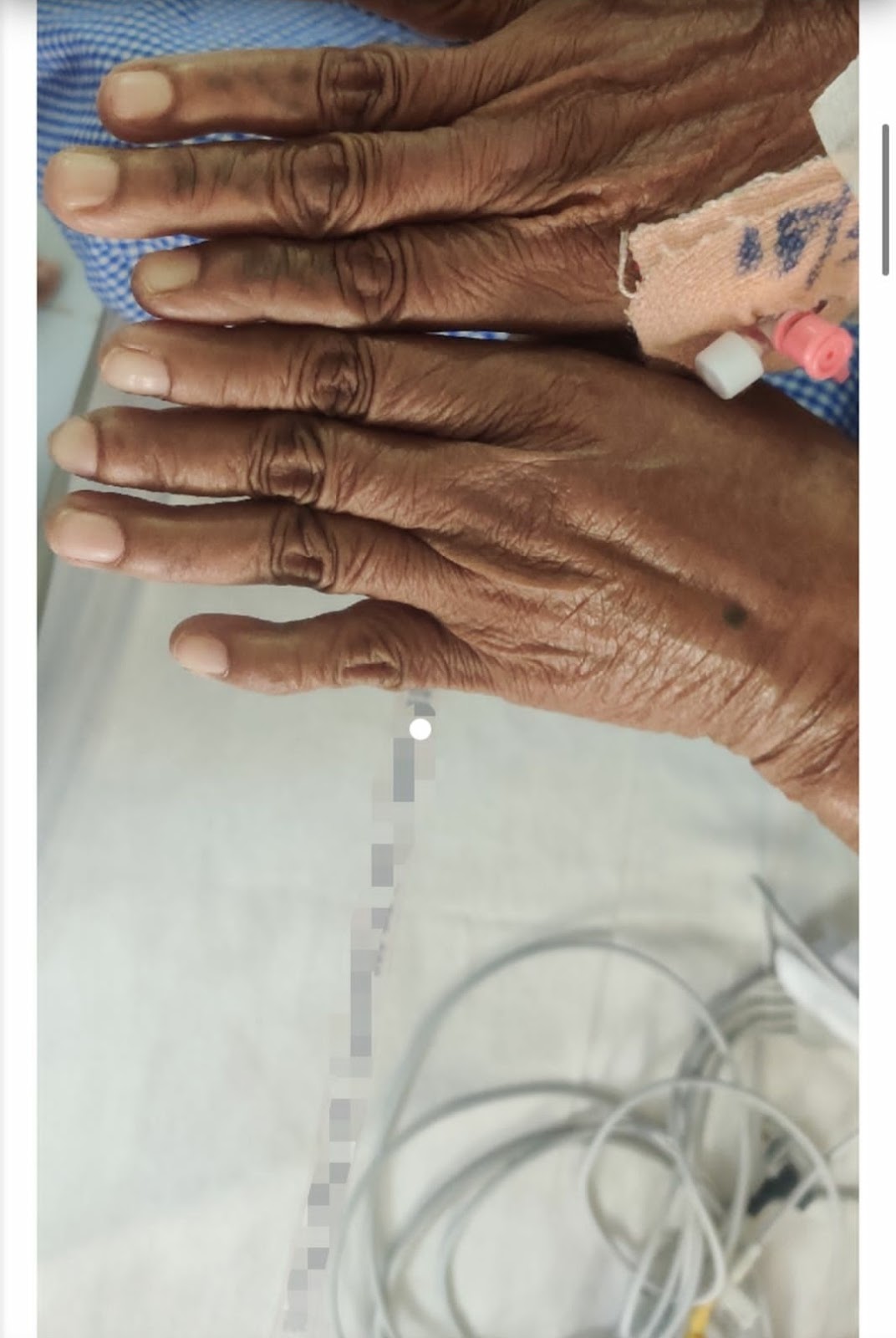
SKIN: HYPERPIGMENTED ULCERATIONS + MACULES ALL OVER THE BODY with local rise of temperature








Vitals:
Temp: febrile

BP
Heart rate 110 bpm
Resp Rate 16/min
SYSTEMIC EXAMINATION
RESPIRATORY SYSTEM:
I: Chest bilaterally symmetrical, all quadrants
moves equally with respiration
P: Trachea central, chest expansion normal
P: Resonant
A: B/l equal air entry, no added sounds
CVS EXAMINATION:
I: No precordial buldge. Apical impulse
visible, Venous prominence
P: Apical impulse, No palpebral pulsation.
thrill
A: S1 S2, No murmur
ABDOMINAL EXAMINATION:
Abdomen is soft and non tender
No organomegaly
No shifting dullness
No fluid thrill
Bowel sounds heard
ABNORMAL INVESTIGATION FINDING
1) pancytopenia
2)RAISED ESR
3) decreased total protein and albumin











Differential: Methotrexate toxicity ?
SLE( anti phospholipid antibody syndrom?)
DISCUSSION:
Reference:
1) https://link.springer.com/article/10.1007/s13555-014-0056-z
most cases of methotrexate-induced ulceration have been reported in patients with psoriasis on low-dose treatment rather than in those on high-dose oncology regimens
It is postulated that that the increased proliferation of keratinocytes within psoriatic plaques makes them particularly vulnerable to the effects of folate-antagonism.
Lawrence and Dahl described two patterns of methotrexate-induced ulceration: type 1 as superficial ulceration of existing psoriatic plaques and type 2 as ulceration of non-psoriatic skin.
Diagnosis:
Diagnostic biopsy is rarely required, however, histological features of methotrexate-induced ulceration include swollen keratinocytes with diminished nuclear and cytoplasmic staining and occasional vacuolated or dyskeratotic cells indicative of incipient epidermal necrosis
Treatment:
In cases of ulceration, withdrawal of methotrexate supported by skin-directed therapy usually leads to rapid improvement in ulceration with many patients showing signs of healing within a few days; however, in isolated cases ulceration persists for years
Prevention:
Pharmacogenomic evaluation of methotrexate may allow for future pre-treatment testing for risk of efficacy and toxicity.

Comments
Post a Comment